As researchers improve ways to quickly and cheaply sequence DNA, the concept of precision medicine is gaining a foothold in the medical community. When it comes to cancer, a disease that leaves its mark in a patient’s genome, sequencing tumor DNA to tailor treatment plans to individuals seems an obvious application of the technology. “The idea of precision medicine as in individualized treatment, I think that makes so much sense,” says Alice Soragni, a cancer biologist at the University of California, Los Angeles (UCLA) David Geffen School of Medicine. “When you work with a few of these tumors, each and every one is a bit different.”
Over the past few years, the field of oncology has shifted in this direction. In 2017, the US Food and Drug Administration (FDA) approved the first cancer treatment for patients whose tumors carry a specific genetic signature. Today, there are dozens of genetic tests used to inform decisions for some 40 different treatments for diverse cancer types. But in lots of cases, tumor DNA doesn’t hold any clues that researchers can yet make sense of, Soragni says. “If you find those [actionable targets] that’s great. But what about everyone else?”
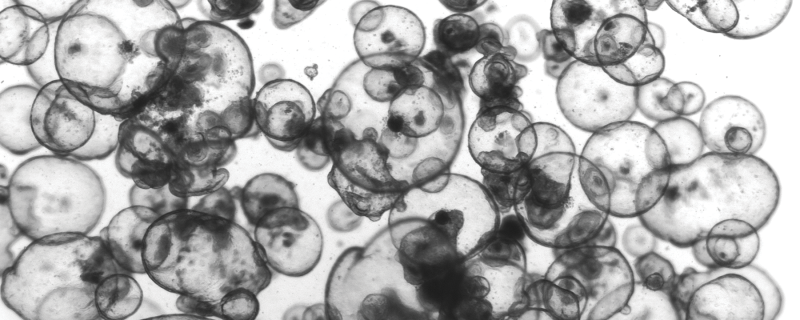
An alternative way to try to forecast treatment responses is to subject animal or cellular models of a patient’s cancer to drug screens in the lab. Relatively new to this scene are organoids, three-dimensional balls of tumor cells that grow in beads of gel or in special plates that the cells cannot attach to. Since 2011, researchers have developed organoids of numerous cancer types, including breast, prostate, liver, pancreatic, and brain, and have demonstrated these models’ ability to recapitulate aspects of in vivo biology. “This is an exciting technology,” says Columbia University molecular geneticist Michael Shen, who last year published a description of the first bladder cancer organoids. “Right now, it’s all the rage.”
Researchers are hopeful that tumor organoids will help predict patient drug responses and support the personalization of treatment plans. In one 2018 study, for example, researchers subjected several dozen patient-derived tumor organoids to the same therapies that the patients actually received and found that the organoids’ responses forecasted when the drugs wouldn’t work in patients 100 percent of the time, and when a treatment would work in almost 90 percent of cases (Science, 359:920–26). “The Science paper is the first to actually compare patient response with organoid sensitivity,” says Jarno Drost, a cancer biologist at the Princess Máxima Center for Pediatric Oncology in the Netherlands who did not participate in the study.
One advantage of 3-D organoids is that they reflect the heterogeneity of a tumor better than 2-D cell cultures, where only a handful of many thousands of patient-derived cancer cells will survive, essentially selecting for those cells that best withstand the 2-D conditions of a petri dish or flask. And compared to xenograft mice carrying tumors developed from a person’s cancer cells, organoids take less time to develop, allowing researchers to conduct drug screens on a much larger scale, says Noah Shroyer, a stem cell and cancer biologist at Baylor College of Medicine in Houston. (See “My Mighty Mouse,” The Scientist, April 2015.)
“It takes months, literally, to grow up enough xenografts in order to do a clinical treatment, a trial, and then you might be able to test only one or two drugs,” Shroyer says. “Theoretically, if you could establish enough organoids, you could test a lot of different drugs” in a clinically relevant time period. “That’s, I think, the unique advantage of the organoids.”
To expedite organoid growth and testing as much as possible, Soragni and her colleagues recently developed a new automatable system that could grow organoids from ovarian cancer cells obtained during surgical resections (Commun Biol, 2:78, 2019). By directly seeding the organoids with patient tumor cells, as opposed to cell lines established from those cells, the approach saves time—it takes just a week to go from surgery to results—and avoids selection of the cells during passaging, Soragni says.
Her team’s approach also bypasses a common problem researchers face when changing media and delivering reagents to organoids: that cell bundles are “just very sticky,” she says, meaning that pipetting things in and out can “introduce all these little errors.” So, instead of seeding the cells to grow up into organoids within a lump of gel in the middle of a plate’s wells, the team put them around the perimeter, so that spherical tumor organoids would grow clear of the center where pipette tips go in and out. Using the new system, Soragni and her colleagues tested two concentrations of 240 different kinase inhibitors in thousands of tumor organoids derived from four patients—three with ovarian cancer and one with tumors in the peritoneum.
The study demonstrates that “you can use this for a relatively large, high-throughput screen that would allow you to uncover novel potential therapeutic angles,” says Shroyer, who did not participate in the study. He adds, however, that using cells taken from patients’ tumors, rather than culturing cell lines established from those tumor cells, requires substantial amounts of patient tissue. In the case of tumor resection, that’s not an issue, but for small biopsies, tissue is precious, and “the pathologist still needs their piece to do the appropriate pathologic diagnosis,” Shroyer notes. In those cases, establishing cell lines is necessary “for ensuring reproducibility of experiments and for pursuing further analyses,” says Shen.
As researchers refine tumor organoid protocols, doctors and patients are anxious for more validation studies like the 2018 Science paper. “Particularly for rare cancers, where there is so little information available, [oncologists] really are interested in knowing, in having some guidance” on how to treat a disease for which there may be no standard of care, says Soragni, an officer at the nonprofit Society for Functional Precision Medicine, which promotes the use of lab-based assays to aid treatment selection for cancer patients.
In addition to seeking clinical validation of these models, researchers are starting to develop organoids that are co-cultured with cancer-associated fibroblasts and macrophages to better recapitulate the in vivo environment. “In a couple of years, I think there will be co-culture conditions that reflect the tumor even better in a microenvironment,” says Drost.
With all the excitement surrounding tumor organoids, their use as models for personalizing cancer therapy could soon become a reality. “To some extent there’s something of a fad about it,” says Shen, “but we’re not working on it because it’s a fad.”